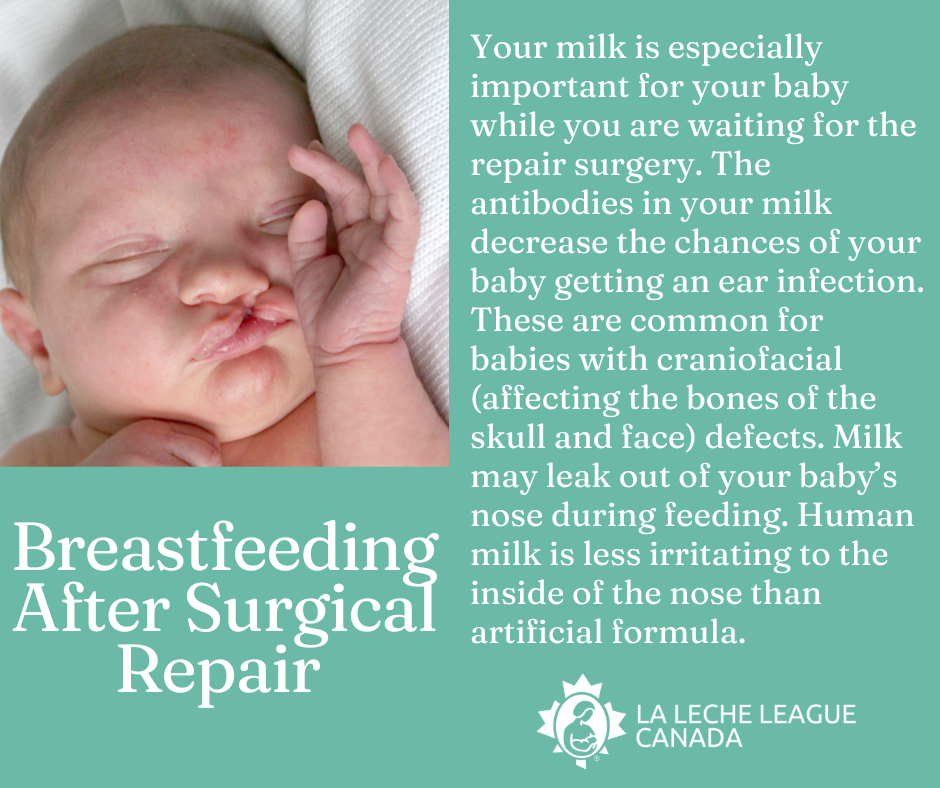
If your baby is born with a cleft lip or palate, you may be told that breastfeeding is not going to be possible. Depending on the position and severity of the cleft you may discover that you can breastfeed. However, it may look different than imagined. An IBCLC (International Board Certified Lactation Consultant) can help you create a breastfeeding plan. It may take time for you and your baby to figure out if breastfeeding will be possible. Feeding your baby your expressed milk is always an option while you are learning to feed at the breast. Or you may continue to feed your baby your expressed milk long-term if feeding at the breast is not possible, or if that is your preference.
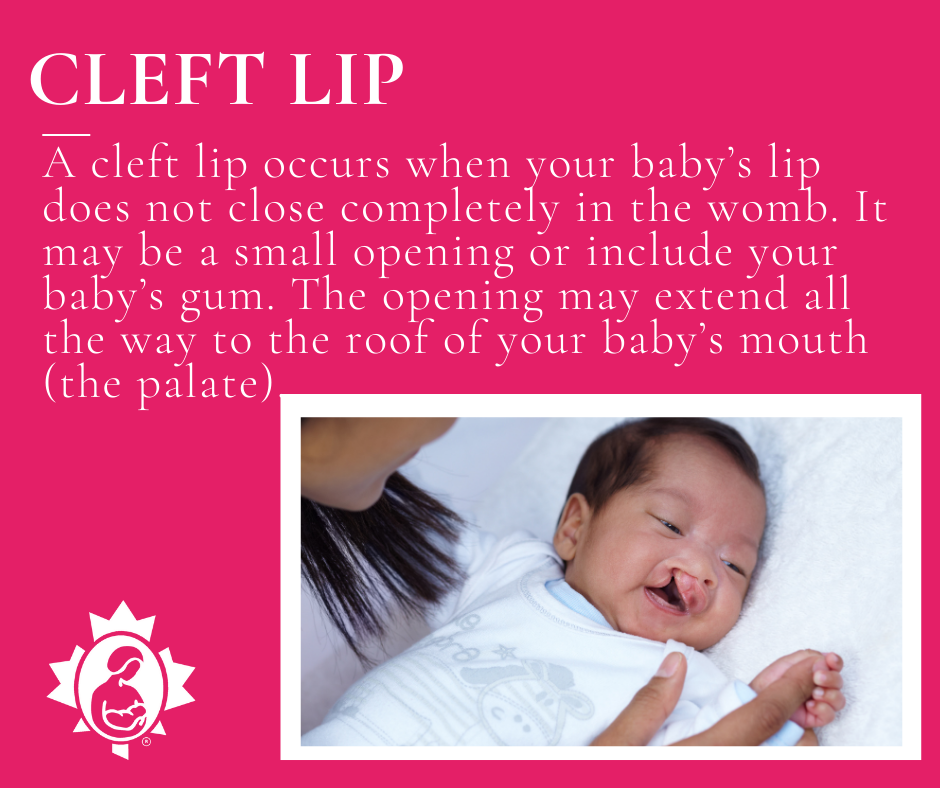
Cleft lip and cleft palate are openings or splits in the upper lip, the roof of the mouth (palate) or both. They occur in the womb when your unborn baby is developing. They are among the most common birth defects and will be surgically repaired when your baby is old enough for the surgery.